Fungal Acne vs Closed Comedones: Spot the Difference
They look nearly identical — small, uniform bumps that refuse to budge. But fungal acne and closed comedones are not the same condition, and treating one with the other's remedy makes things worse, not better.
Here's the core difference: fungal acne (Malassezia folliculitis) is a yeast infection inside hair follicles. It itches, clusters symmetrically, and worsens with antibiotics. Closed comedones are non-inflammatory pore blockages — no infection, no itch, just trapped sebum and dead skin cells that salicylic acid and retinoids can clear. Getting this distinction right is the only path to skin that actually improves.
At a Glance — The Three Fastest Ways to Tell Them Apart
- Itch test: Fungal acne itches, especially after sweating. Closed comedones don't.
- Uniformity test: Fungal acne bumps are nearly identical in size (1–2mm). Closed comedones vary.
- Treatment response test: Closed comedones improve with salicylic acid. Fungal acne doesn't — and may worsen with standard acne products.
Fungal acne and closed comedones look strikingly similar on the surface, but they form through completely different processes. Fungal acne develops when yeast overgrows in hair follicles, triggering inflammation, while closed comedones form when dead skin cells and sebum trap inside pores without infection.
Key Takeaways
- Fungal acne is caused by yeast overgrowth, not bacteria or clogged pores
- Closed comedones are non-inflammatory bumps formed by trapped sebum and skin cells
- Fungal acne typically appears as uniform, itchy clusters, often on the forehead, chest, and back
- Closed comedones are isolated bumps without itching, commonly on the face
- Treatment approaches differ completely between the two conditions
- Misidentifying one for the other leads to ineffective treatment and prolonged frustration
What Are Closed Comedones?
Closed comedones, commonly called whiteheads, are small flesh-colored or white bumps that form when a pore becomes completely blocked. Unlike open comedones (blackheads), the pore remains closed at the surface, trapping sebum, dead skin cells, and sometimes bacteria beneath the skin.
The formation process begins when the skin produces excess keratinocytes, the cells that make up the outermost layer of skin. When these cells don't shed properly, they mix with sebum and create a plug inside the follicle. The pore opening remains covered by a thin layer of skin, which is why closed comedones don't oxidize and turn dark like blackheads.
This type of acne is non-inflammatory, meaning there's no active infection or significant immune response. The bumps feel firm to the touch and don't cause pain or redness unless they become irritated or progress into inflammatory acne.
What Is Fungal Acne?
Fungal acne, technically called Malassezia folliculitis or Pityrosporum folliculitis, isn't actually acne at all. It's a fungal infection of the hair follicles caused by an overgrowth of yeast that naturally lives on everyone's skin.
Under normal circumstances, Malassezia yeast exists harmlessly on the skin surface. When conditions become favorable for yeast proliferation, such as increased oil production, humidity, sweating, or a disrupted skin microbiome, the yeast population explodes. The yeast migrates into hair follicles and triggers an inflammatory immune response.
Your immune system recognizes the overgrowth as a threat and sends inflammatory cells to the area. This creates clusters of small, uniform pustules that look remarkably similar to bacterial acne or closed comedones, but the underlying cause is completely different.
Comedonal Acne vs Fungal Acne: Understanding the Terminology
Many people searching for "comedonal acne" are actually looking at the same condition from a different angle — and confusing it further with fungal acne.
Comedonal acne is the umbrella term dermatologists use for acne dominated by comedones — both open (blackheads) and closed (whiteheads). It is non-inflammatory acne caused by pore blockages, not infection. Closed comedones are one type of comedonal acne.
Fungal acne is not a form of comedonal acne at all. It isn't in the acne family by mechanism. The term "fungal acne" is a popular shorthand for Malassezia folliculitis — a yeast infection of hair follicles that happens to produce bumps resembling comedonal acne.
| Term | What It Actually Is | Caused By |
|---|---|---|
| Comedonal acne | Acne dominated by pore blockages | Excess sebum + dead skin cells |
| Closed comedones | Non-inflammatory blocked pore (whitehead) | Trapped sebum under intact skin |
| Fungal acne | Malassezia folliculitis (yeast infection) | Yeast overgrowth in hair follicles |
| Bacterial acne | Inflammatory acne (papules, pustules) | C. acnes bacteria in blocked pores |
The practical takeaway: if your bumps are uniform, itchy, and haven't responded to standard comedonal acne treatments (salicylic acid, retinoids), reclassify them as potential fungal acne rather than stubborn comedonal acne.
Visual Differences: What You Actually See
Understanding the visual distinctions helps narrow down which condition you're dealing with, though these observations should never replace professional evaluation.
| Feature | Fungal Acne | Closed Comedones |
|---|---|---|
| Appearance | Uniform small bumps, often pustular | Varying sizes, flesh-colored bumps |
| Distribution | Clusters, symmetrical patterns | Scattered, isolated bumps |
| Common locations | Forehead, chest, back, shoulders | Face (especially chin, forehead) |
| Itching | Frequently itchy | Rarely itchy |
| Size consistency | Very uniform (1–2mm) | Variable sizes |
Fungal acne typically appears as monomorphic lesions, meaning all the bumps look nearly identical in size and appearance. This uniformity happens because the yeast triggers a consistent inflammatory response across affected follicles.
Closed comedones show more variation because they develop independently based on individual pore behavior, sebum production levels, and localized skin cell turnover rates. You might see tiny bumps alongside larger ones within the same area.
The Itch Factor: A Telling Difference
One of the most distinctive differences between these conditions is the presence of itching. Fungal acne frequently causes noticeable itchiness because the immune system actively fights the yeast overgrowth. The inflammatory mediators released during this process stimulate nerve endings in the skin, creating that characteristic itch.
The itching often worsens after sweating, wearing occlusive clothing, or in humid environments because these conditions encourage further yeast proliferation. Some people describe the sensation as a crawling or tingling feeling rather than a sharp itch.
Closed comedones rarely itch because there's no active infection or significant inflammatory response. The blockage exists passively within the pore without triggering immune activation. If a closed comedone becomes itchy, it may indicate progression to inflammatory acne or external irritation from products or friction.
Location Patterns: Where They Appear
While both conditions can theoretically develop anywhere you have hair follicles and sebaceous glands, their preferred locations differ significantly.
Fungal acne thrives in areas with high sebum production, warmth, and moisture. The chest, back, shoulders, and forehead are prime locations. Athletes and people who sweat heavily often develop fungal acne along the hairline, between the shoulder blades, and across the upper chest where sweat accumulates and clothing creates occlusion.
The yeast responsible for fungal acne feeds on the fatty acids in sebum and proliferates in warm, moist environments. This explains why the condition often worsens during summer months, after intense workouts, or when wearing tight synthetic fabrics that trap heat and moisture against the skin.
Closed comedones appear most commonly on the face, particularly in areas with dense sebaceous gland concentrations like the forehead, nose, and chin. While they can develop on the body, facial appearance is far more typical. The cheeks, jawline, and around the mouth are frequent sites, especially in people who use heavy moisturizers, foundations, or hair products that migrate onto facial skin.
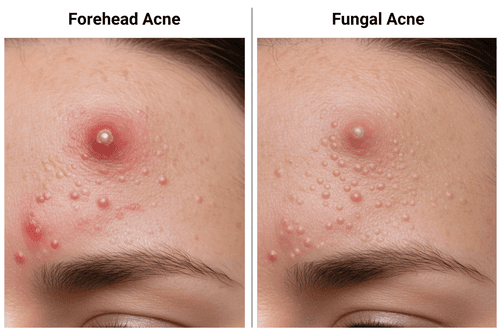
Fungal Acne vs Closed Comedones on the Forehead: Why Location Matters
The forehead is the most common location where these two conditions get confused — and the confusion makes sense. Both produce clusters of small, flesh-toned bumps across the forehead, and both worsen when heavy products (sunscreens, moisturizers, hair products) are applied to the area.
Forehead Closed Comedones — What They Look Like
Closed comedones on the forehead tend to appear along the hairline and T-zone where sebaceous glands are densest. They develop gradually — often over weeks — and vary slightly in size and distribution. Hair products like dry shampoos, hair oils, and pomades that migrate onto the forehead are a leading trigger. The skin texture feels rough but the bumps don't itch.
Forehead Fungal Acne — What It Looks Like
Fungal acne on the forehead appears suddenly, often in a band along the hairline or across the full forehead width. The bumps are strikingly uniform — almost identical in size — and the area frequently feels itchy or tingly. This pattern often emerges after starting antibiotics, using an oil-rich moisturizer, or spending time in heat and humidity.
The Hairline Clue
If the bumps are thickest right at the hairline and extend slightly into the scalp, fungal involvement is more likely. Malassezia thrives in the follicle-dense, sebum-rich hairline environment. Closed comedones rarely concentrate along the hairline itself — they tend to sit on the forehead skin above the brow.
Quick forehead test: Press a piece of clear tape gently onto the bump cluster, then examine under a bright light. Closed comedones may leave a faint sebum imprint on the tape. Fungal acne does not — the follicle involvement is too deep for tape-stripping to capture. This isn't diagnostic but offers one additional data point.
Products That Worsen Each Condition — What to Avoid
Malassezia yeast feeds specifically on certain fatty acids found in many common skincare ingredients. Using the wrong product can take a manageable flare and turn it into weeks of persistent bumps.
Ingredients That Feed Malassezia (Avoid with Fungal Acne)
Research has identified specific fatty acid profiles that Malassezia metabolises most aggressively [1]. Oils and ingredients high in C11–C24 fatty acids are the primary culprits:
- Coconut oil — high in lauric acid (C12), a known Malassezia substrate
- Olive oil, argan oil, marula oil — oleic acid (C18:1) content feeds yeast proliferation
- Flaxseed oil and hemp seed oil — linoleic acid-heavy but still carry problematic fatty acids
- Fatty alcohol-heavy moisturisers — ingredients like cetearyl alcohol and stearyl alcohol in high concentrations
- Heavy occlusive creams — not inherently fungal-feeding, but create the warm, moist environment Malassezia thrives in
- Fermented skincare ingredients — certain ferments can promote yeast growth on susceptible skin
Safer alternatives for fungal acne-prone skin: Squalane (derived from sugarcane), mineral oil, dimethicone, and niacinamide serums are generally considered Malassezia-safe and won't feed yeast overgrowth.
Ingredients That Worsen Closed Comedones (Avoid with Blocked Pores)
Closed comedones worsen with ingredients rated high on the comedogenicity scale — those that encourage pore blockage:
- Isopropyl myristate — one of the most comedogenic ingredients in skincare
- Algae and seaweed extracts — commonly comedogenic for pore-prone skin
- Cocoa butter and shea butter — rich emollients that can occlude follicles
- Sodium lauryl sulphate (SLS) — disrupts the skin barrier, triggering compensatory sebum overproduction
- Heavy silicones at high concentrations — can trap sebum beneath the skin surface
- Oil-heavy sunscreens — particularly chemical sunscreens in cream form without non-comedogenic formulation
Citable one-liner: The oils that damage a comedone-prone complexion are different from the oils that feed fungal acne — but many products contain both types of problematic ingredients simultaneously.
[1] Prohic A, et al. Malassezia species in healthy skin and in dermatological conditions. International Journal of Dermatology. 2016;55(5):494–504.
How to Treat Each Condition: A Practical Guide
Treating Closed Comedones: Step-by-Step
Step 1 — Introduce a chemical exfoliant (weeks 1–4)
Salicylic acid (BHA) at 0.5%–2% is the most effective first-line ingredient for closed comedones. It is oil-soluble, which means it penetrates the pore lining and dissolves the sebum-cell plug from the inside. Apply a salicylic acid toner or serum once daily to start, increasing to twice daily after two weeks if no irritation occurs.
Step 2 — Add a retinoid (weeks 4–8)
Retinoids (adapalene 0.1% is widely available over the counter; tretinoin requires a prescription) accelerate cell turnover, which prevents dead skin cells from accumulating inside the follicle. Start two to three nights per week to avoid irritation. Most people see a visible reduction in comedone size within six to eight weeks of consistent retinoid use.
Step 3 — Audit your skincare for comedogenic ingredients (ongoing)
Remove any products with isopropyl myristate, heavy butters, or SLS. Switch to a non-comedogenic, lightweight moisturiser with ceramides or hyaluronic acid.
Step 4 — Protect with a non-comedogenic SPF (daily)
UV damage slows cell turnover and increases sebum oxidation — both of which worsen closed comedones. A light, fluid SPF 30–50 used every morning supports the exfoliation work happening beneath the surface.
Expected timeline for closed comedones: Visible improvement in 4–6 weeks with salicylic acid; significant clearance in 8–12 weeks with a combined BHA + retinoid routine.
Treating Fungal Acne (Malassezia Folliculitis): Step-by-Step
Step 1 — Confirm the diagnosis before treatment
The most important step. Using antifungal treatment on bacterial acne does nothing; using it on closed comedones does nothing. Confirm with the itch test, antibiotic history test, and if possible a KOH microscopy test from a dermatologist.
Step 2 — Start antifungal treatment (weeks 1–2)
Ketoconazole 2% shampoo (used as a face or body wash, left on for 2–3 minutes before rinsing) is the most commonly recommended first-line antifungal for Malassezia folliculitis. Zinc pyrithione shampoo used similarly is an alternative for milder cases. Use daily for the first two weeks.
Step 3 — Strip back your skincare routine (weeks 1–4)
Remove all oil-heavy products, fermented ingredients, and occlusive creams. Simplify to: a gentle, sulphate-free cleanser, a Malassezia-safe moisturiser (squalane or mineral oil base), and SPF.
Step 4 — Address contributing lifestyle factors (ongoing)
Change out of sweaty gym clothes promptly. Shower after workouts. Choose breathable, natural-fibre fabrics. Avoid long periods in hot, humid environments without cleansing afterward.
Step 5 — Maintain with antifungal shampoo twice weekly (from week 4)
Once the active flare resolves, twice-weekly ketoconazole wash maintenance significantly reduces recurrence rates, particularly in humid climates or during summer months [2].
Expected timeline for fungal acne: First visible improvement in 1–2 weeks with antifungal treatment; significant clearance in 3–4 weeks; full resolution in 6–8 weeks with consistent treatment and trigger elimination.
Citable one-liner: Fungal acne typically clears in 3–4 weeks with antifungal treatment; closed comedones require 8–12 weeks of combined BHA and retinoid use.
What the Research Says: Key Data on Both Conditions
Understanding what the clinical literature actually says about both conditions helps set realistic expectations — and explains why accurate diagnosis matters so much.
On Malassezia prevalence
Malassezia yeast is present on the skin of virtually all healthy adults. Studies show it constitutes up to 80% of the fungal microbiome on sebaceous skin sites including the scalp, face, and upper chest [3]. Overgrowth, not presence, is the problem.
On fungal acne misdiagnosis rates
Malassezia folliculitis is consistently reported as one of the most frequently misdiagnosed skin conditions in dermatology outpatient settings. A 2017 review in Dermatology and Therapy noted that many cases are initially treated as bacterial acne, leading to antibiotic exposure that worsens the underlying yeast overgrowth [4].
On salicylic acid efficacy for comedonal acne
A double-blind randomised controlled trial found that 2% salicylic acid applied twice daily produced a statistically significant reduction in closed comedone count within four weeks compared to vehicle control. By week eight, reduction rates exceeded 50% in compliant participants [5].
On ketoconazole for Malassezia folliculitis
A systematic review found topical ketoconazole (1–2%) to be effective in resolving Malassezia folliculitis in 70–80% of cases within four weeks of consistent use, with low rates of recurrence when maintenance treatment was continued [6].
On the antibiotic-fungal acne link
Multiple case series document new-onset Malassezia folliculitis appearing within two to six weeks of starting broad-spectrum antibiotic therapy. The mechanism — depletion of skin bacterial flora that naturally compete with Malassezia — is well established [4].
[5] Arif T. *Salicylic acid as a peeling agent: a comprehensive review.* Clinical, Cosmetic and Investigational Dermatology. 2015;8:455–61.
Frequently Asked Questions
Can you have fungal acne and closed comedones at the same time?
Yes — and it's more common than most people expect. Both conditions can coexist on the same area of skin, particularly the forehead and T-zone. The practical approach: treat the fungal component first (2–4 weeks of antifungal), then address remaining non-itchy, uniform bumps with salicylic acid. If clearing the fungal acne reveals a separate pattern of flesh-coloured varying bumps, those are likely closed comedones requiring their own treatment.
Why does fungal acne get worse after antibiotics?
Antibiotics eliminate bacterial populations on your skin — including the bacteria that naturally compete with Malassezia yeast for resources inside hair follicles. Without that bacterial competition, yeast proliferates rapidly and migrates deeper into follicles. This is why new or worsening clusters of uniform itchy bumps after a course of antibiotics (for acne or any other reason) should prompt a reassessment toward Malassezia folliculitis rather than more antibiotic treatment.
How long does it take for closed comedones to clear?
With consistent use of salicylic acid (2% BHA) once or twice daily, most people see visible reduction in closed comedone density within four to six weeks. Adding a retinoid such as adapalene 0.1% accelerates clearance — expect significant improvement at the eight-to-twelve-week mark. Consistency matters more than concentration: using a lower-strength product daily outperforms a higher-strength product used sporadically.
Is niacinamide safe to use if you have fungal acne?
Niacinamide is generally considered Malassezia-safe. It doesn't contain the fatty acid substrates that Malassezia metabolises, and it helps regulate sebum production — one of the underlying conditions that enables yeast overgrowth. It can be used alongside antifungal treatment without concern. Look for a water-based niacinamide serum without added oils or fermented ingredients.
Why doesn't salicylic acid clear fungal acne?
Salicylic acid works by dissolving the sebum-cell plug inside a blocked pore — a mechanism specific to comedonal acne. Fungal acne isn't a pore blockage. It's an inflammatory yeast infection inside the follicle wall. Salicylic acid has no antifungal activity, so it cannot address the underlying Malassezia overgrowth. Some people see temporary surface-level improvement (BHA's anti-inflammatory properties) without actual resolution, which often leads to months of ineffective treatment.
Can fungal acne scar?
Fungal acne rarely causes the deep scarring associated with nodular or cystic bacterial acne, because the inflammatory response — while present — is typically confined to the upper follicle and doesn't penetrate deeply into the dermis. However, post-inflammatory hyperpigmentation (PIH) — dark marks left after inflammation resolves — is common, particularly in medium-to-deep skin tones. These marks are not scars and generally fade within three to six months with consistent SPF use.
What SPF is safe to use with fungal acne?
Mineral sunscreens containing zinc oxide or titanium dioxide as active ingredients are generally Malassezia-safe. Choose lightweight fluid or gel textures without added plant oils. Avoid chemical sunscreen formulas in heavy cream bases that contain coconut oil, olive oil, or squalane listed high on the ingredient list (though squalane from sugarcane at low concentrations is generally considered safe). A non-comedogenic, oil-free SPF 30–50 mineral formula is the safest default for fungal acne-prone skin.
What This Means for You
Getting this diagnosis right changes everything. If you treat fungal acne with salicylic acid and retinoids, you'll spend months seeing no improvement — or making the yeast environment worse. If you treat closed comedones with antifungal washes, you'll strip your skin unnecessarily while the real pore-clearing work never happens. Most people who've been stuck with 'stubborn acne' that won't shift are dealing with a misidentification problem, not a treatment-resistance problem.
Start with the three tests — itch, uniformity, and antibiotic history. They take seconds and will point you toward the right starting point before you spend another month on the wrong product.
Your next steps:
- Do the itch test right now. Touch the bump cluster gently. Does it itch or tingle, especially after sweating? If yes, investigate fungal acne first.
- Check your antibiotic history. Did these bumps appear or worsen within six weeks of finishing antibiotics? If yes, Malassezia folliculitis is the most likely cause.
- Audit your current skincare for the ingredients listed above. Oils like coconut, olive, and argan actively feed yeast — removing them costs nothing and provides immediate evidence within two to four weeks.
- Start with one targeted treatment. Ketoconazole shampoo for fungal acne, 2% salicylic acid for closed comedones — not both simultaneously — so you can clearly read your skin's response.
- Give treatment a real timeline. Fungal acne should respond within three to four weeks of consistent antifungal use. Closed comedones need eight to twelve weeks of BHA + retinoid. If nothing changes within those windows with consistent treatment, a dermatologist can run a definitive KOH test.
If home identification and over-the-counter treatment aren't producing results after the timelines above, that's the signal to seek a professional diagnosis. A KOH microscopy test takes minutes and removes all guesswork.
Editorial Standards
Clear Ritual has Strict sourcing guidelines to ensure our content is accurate and current. We rely on peer-reviewed studies, academic research institutions, and medical associations. We strive to use primary sources and refrain from using tertiary references. See a mistake? Learn More about our Editorial Standards.
Related Articles
Antibiotics and Fungal Acne: Understanding the Link
Published April 22, 2026

Forehead Acne vs Fungal Acne: Differences in Causes and Treatment
Published May 24, 2026
Do You Have Fungal Acne? Here's How It's Different From Bacterial Breakouts
Published April 22, 2026

Fungal Acne: Causes, Symptoms, Treatment & Prevention Tips
Published May 14, 2026
