Pimple vs Acne: What’s the Real Difference?
H1: Pimple vs Acne: What’s the Real Difference?
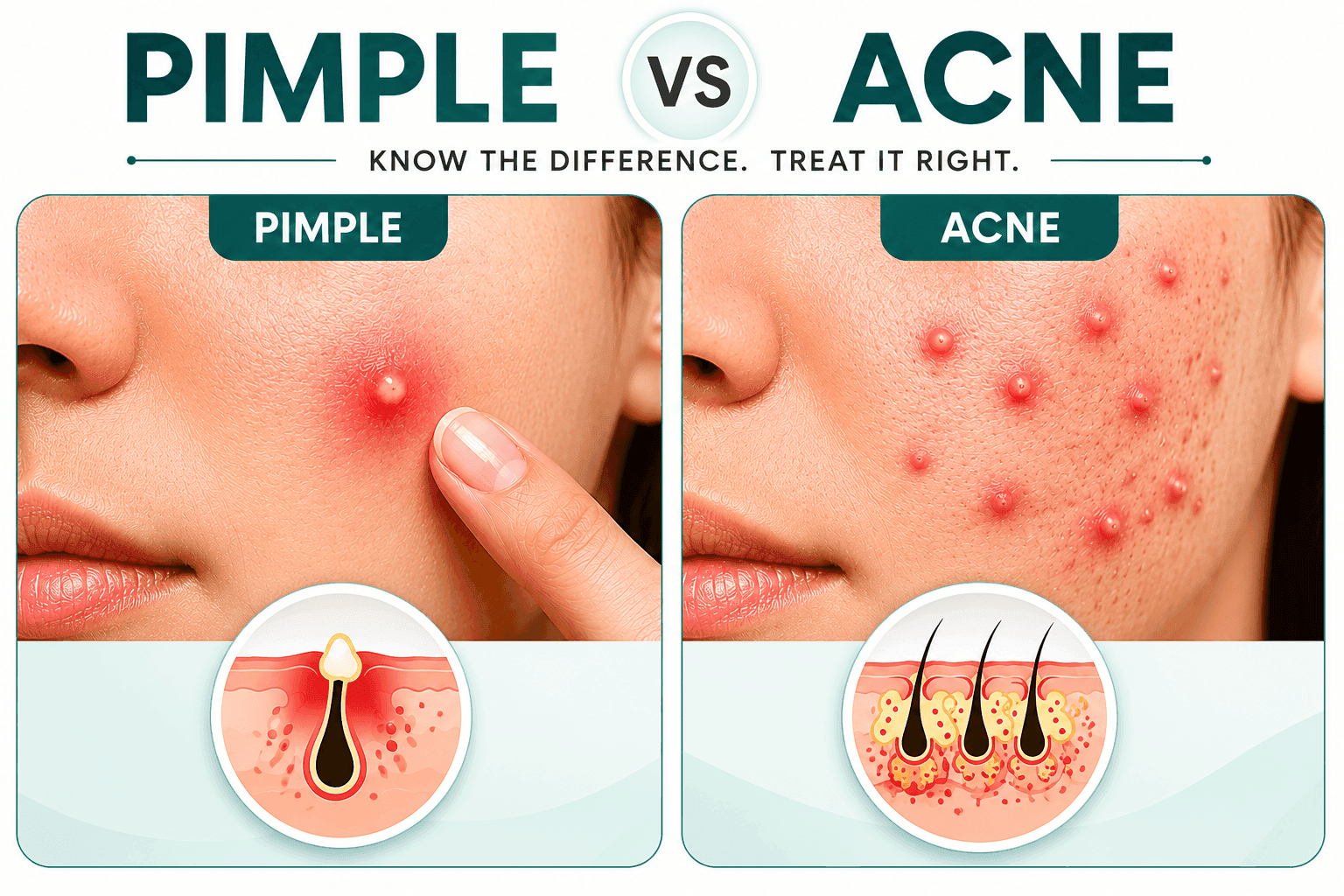
Acne vs pimples vs zits is a common confusion, but a pimple and acne are not the same thing, even though people use the words interchangeably. A pimple is a single blocked, inflamed pore, while acne is the chronic skin condition that keeps producing those pimples over and over, across multiple areas of your face or body. Think of it this way: a pimple is a symptom, acne is the diagnosis. A zit is just slang for a pimple, the same blocked, inflamed pore with a different name.
Acne vs Pimples vs Zits: The Quick Answer
No, a pimple and acne are not the same thing, even though people use the words interchangeably. A pimple is a single blocked, inflamed pore. Acne is the chronic skin condition that keeps producing those pimples, over and over, across multiple areas of your face or body.
Think of it this way: a pimple is a symptom. Acne is the diagnosis.
If your skin breaks out occasionally, one spot after a stressful week, one whitehead before your period, you are most likely dealing with isolated pimples. If you consistently see multiple lesions at different stages [some healing, some new] and your skin never fully clears for weeks at a time, that pattern is acne.
The fastest way to tell them apart:
- Frequency: one pimple now and then vs. breakouts that keep coming back
- Number: one or two lesions vs. multiple across your face, chest, or back
- Duration: clears in a few days vs. cycles that last weeks or months
- Recovery: skin returns to normal vs. skin never fully clears between breakouts
A zit, for the record, is just slang for a pimple, the same blocked, inflamed pore with a different name. See the full breakdown below.
A pimple is a single inflamed lesion caused by a clogged pore, while acne is a chronic skin condition involving repeated breakouts across multiple areas. Both involve sebum, bacteria, and inflammation, but acne reflects an ongoing cycle that requires different management than an occasional pimple.
Key Takeaways:
- A pimple: is one blocked pore that becomes inflamed.
- Acne: is a recurring condition with multiple lesions over time.
- Biology: both share the same biological process but differ in frequency and severity.
- Care approach: understanding the difference helps determine the right care approach.
- Persistent breakouts: signal acne, which may need professional evaluation.
What Happens When a Pore Gets Blocked
Every pore on your face connects to a sebaceous gland that produces sebum, an oily substance that protects and moisturizes skin. When dead skin cells, sebum, and debris accumulate inside a pore, they create a plug. This blockage traps oil and creates an environment where Cutibacterium acnes bacteria multiply rapidly.
The immune system responds to this bacterial overgrowth by sending white blood cells to the area, triggering inflammation. The result is redness, swelling, and sometimes pus formation. This process occurs whether you develop a single pimple or chronic acne, but the frequency and pattern determine which term applies.
What Defines a Pimple
A pimple represents an isolated incident. You might notice one inflamed bump on your chin after a stressful week, or a whitehead on your forehead following a sweaty workout. The skin issue resolves within days to a week, then your complexion returns to its baseline state.
Pimples often appear in response to temporary triggers. Touching your face transfers bacteria and oils from your hands to your pores. Wearing a face mask for extended periods creates friction and traps moisture against skin, leading to localized breakouts. A high-sugar meal can spike insulin levels, which temporarily increases oil production and inflammation.
These occasional blemishes do not indicate an underlying skin disorder. Most people experience random pimples throughout their lives without developing a chronic condition.
What Qualifies as Acne
Acne describes a persistent pattern of breakouts involving multiple lesions across different stages of development. When you consistently see whiteheads, blackheads, papules, pustules, nodules, or cysts appearing on your face, chest, or back over weeks and months, you are dealing with acne rather than isolated pimples.
Dermatologists classify acne by severity. Mild acne involves mostly non-inflamed comedones with occasional small papules. Moderate acne includes more widespread inflammation with regular pustules. Severe acne presents as deep, painful nodules and cysts that affect larger areas and carry higher risk for scarring.
The condition reflects ongoing dysfunction in how your skin produces and sheds cells, regulates sebum, and manages bacterial populations. Hormonal fluctuations, genetic predisposition, and chronic inflammation keep the cycle active rather than allowing skin to stabilize between breakouts.
The Biological Differences
While both pimples and acne involve the same basic mechanism of pore blockage and inflammation, the underlying skin behavior differs significantly.
With occasional pimples, your sebaceous glands function normally most of the time. A temporary trigger causes one or two pores to become blocked, inflammation develops, and then the skin heals without further incident. The protective barrier remains intact, cell turnover stays balanced, and sebum production returns to baseline.
Acne involves chronic dysregulation. Sebaceous glands may overproduce oil continuously due to hormonal sensitivity, particularly to androgens like testosterone. The follicular lining sheds cells abnormally fast, creating more debris that mixes with excess sebum. This combination forms microcomedones that develop into visible lesions repeatedly.
The skin microbiome also plays a role. Everyone has C. acnes bacteria on their skin, but people with acne often show altered bacterial populations and increased inflammatory response to these organisms. The immune system stays activated, maintaining low-grade inflammation even between visible breakouts.
What the Research Says: Evidence Behind Acne vs Pimples
The biology behind acne and pimples is well documented. Here is what peer-reviewed research confirms.
Sebum and follicular hyperkeratinisation are the primary drivers
A landmark review in Nature Reviews Disease Primers confirmed that all acne lesions, from a single pimple to widespread cystic acne, begin with the same event: abnormal shedding of follicular keratinocytes combined with excess sebum production. The difference between an isolated pimple and chronic acne is whether this process resets or continues cycling.
Hormones determine chronicity
Androgenic hormones, particularly testosterone and dihydrotestosterone [DHT], bind to receptors in sebaceous glands and increase oil output. A review in the Journal of Clinical and Aesthetic Dermatology found that androgen sensitivity explains why some people develop chronic acne while others only experience occasional pimples despite similar stress or dietary exposures. This is why hormonal acne, concentrated along the jawline and chin, tends to be more persistent than stress-triggered isolated pimples.
The skin microbiome plays a key role
Cutibacterium acnes [formerly Propionibacterium acnes] is present on every person's skin. Research published in the Journal of Investigative Dermatology found that it is not the presence of C. acnes that distinguishes acne-prone skin from clear skin, it is the specific strains of the bacteria and the immune system's inflammatory response to them. People with chronic acne show heightened innate immune activation even between visible breakouts, which explains why acne is never truly inactive in the way an isolated pimple resolves completely.
Key statistics at a glance:
- Acne prevalence: acne affects approximately 85% of people aged 12-24 at some point.
- Adult acne: roughly 15% of adults continue to experience acne beyond age 25.
- Treatment timeline: spot treatments clear most isolated pimples within 3-5 days; clinical acne treatments require consistent use for 6-12 weeks before measurable improvement.
Common Patterns That Distinguish Them
| Factor | Occasional Pimples | Acne |
|---|---|---|
| Frequency | Random, sporadic | Constant or recurring |
| Number of lesions | One to three at a time | Multiple across different areas |
| Duration | Resolves within days | Ongoing for weeks or months |
| Trigger identification | Usually identifiable | Multiple or unclear factors |
| Response to basic care | Clears with simple treatment | Requires consistent management |
Why Location and Timing Matter
Where and when breakouts appear provides clues about whether you are experiencing isolated pimples or chronic acne.
A single pimple on your jawline appearing the week before your menstrual cycle reflects normal hormonal fluctuation. This pattern occurs predictably and resolves without spreading to other areas. The rest of the month, your skin remains clear.
Acne typically affects areas with the highest concentration of sebaceous glands: the face, particularly the forehead, nose, and chin, along with the chest, shoulders, and upper back. Lesions appear continuously rather than following a predictable monthly pattern. You might clear one area only to develop new breakouts nearby.
Hormonal acne often concentrates along the lower face and jawline, appearing as deep, painful lesions that linger for weeks. This distribution reflects androgen receptor concentration in those areas. The persistence and specific location indicate a chronic hormonal influence rather than temporary factors.
What Amplifies the Condition
Certain behaviors and exposures worsen acne while having minimal impact on occasional pimples.
Over-cleansing strips away the skin's protective lipid barrier, which paradoxically triggers increased oil production as the skin attempts to restore balance. This creates a cycle where excessive washing leads to more sebum and potentially more breakouts.
Harsh physical exfoliation causes micro-tears in the skin, increasing inflammation and potentially spreading bacteria from existing lesions to healthy pores. Chemical exfoliants can help when used appropriately, but aggressive scrubbing damages acne-prone skin.
Occlusive cosmetics and heavy moisturizers trap sebum and bacteria inside pores, particularly in people whose skin already produces excess oil. Non-comedogenic formulations allow the skin to breathe while providing necessary hydration.
Sleep deprivation elevates cortisol, a stress hormone that increases inflammation and oil production. One late night might trigger a random pimple, but chronic poor sleep contributes to persistent acne by keeping the body in a stressed state.
Dietary factors affect individuals differently, but some people notice that dairy products or high-glycemic foods consistently worsen their acne. These foods influence insulin and insulin-like growth factor, which stimulate sebaceous glands and increase inflammation. The connection is less relevant for occasional pimples but can be significant in chronic acne.
How Response to Treatment Differs
An isolated pimple typically responds to spot treatment with benzoyl peroxide or salicylic acid. The inflammation subsides within a few days, and the lesion heals without requiring ongoing intervention. You can resume your normal skincare routine once the blemish clears.
Acne requires sustained management. Topical treatments need consistent application across the entire affected area, not just on visible lesions, because they prevent microcomedones from forming. Results take weeks to become noticeable as the products gradually normalize cell turnover and reduce bacterial populations.
Some people with acne need oral medications that address internal factors like hormonal imbalance or systemic inflammation. These treatments target the underlying processes that keep acne active rather than just managing surface symptoms.
The commitment level differs substantially. Managing occasional pimples involves responding to breakouts as they occur. Treating acne means maintaining a daily regimen even when your skin looks clear, because stopping treatment often allows the condition to return.
Treating Pimples vs Treating Acne: What Actually Works, and What Doesn't
Once you know which one you're dealing with, treatment logic becomes much clearer.
For isolated pimples
Spot treatments work because they target a localised, temporary problem. Look for these active ingredients:
- Benzoyl peroxide [2.5%-5%]: kills C. acnes bacteria directly at the pore. Works in 3-5 days on active lesions.
- Salicylic acid [0.5%-2%]: a beta-hydroxy acid that dissolves the dead skin cell and sebum plug inside the pore.
- Sulfur: reduces inflammation and absorbs excess oil. Gentler than benzoyl peroxide, useful for sensitive skin.
- Tea tree oil [5%]: a plant-derived antimicrobial. A small randomised trial in the Medical Journal of Australia found it as effective as 5% benzoyl peroxide for pimple reduction over three months, with fewer side effects.
Apply a spot treatment directly to the lesion. No need to treat surrounding skin.
For acne
Acne treatment requires whole-area application, not spot treatment. The goal is to prevent microcomedones, the invisible precursor lesions, from forming in the first place.
- Topical retinoids [adapalene, tretinoin]: normalise cell turnover and prevent follicular plugging. Adapalene 0.1% is available OTC in many countries. Expect 8-12 weeks of consistent use before visible improvement.
- Benzoyl peroxide [applied to the full zone, not just spots]: reduces bacterial load across the affected area.
- Niacinamide [4%-5%]: reduces sebum production and calms inflammation. Supported by a study in the International Journal of Dermatology showing comparable efficacy to clindamycin gel for mild-to-moderate inflammatory acne.
- Azelaic acid [15%-20%]: anti-inflammatory, antibacterial, and reduces post-inflammatory hyperpigmentation simultaneously. Useful for acne with residual dark spots.
- Prescription options: for moderate-to-severe acne: topical clindamycin, oral antibiotics, combined oral contraceptives [for hormonal acne in women], or isotretinoin for severe cystic cases. These require a dermatologist.
OTC vs prescription: how to decide
| Acne severity | Appropriate first step | Expected timeline |
|---|---|---|
| Occasional pimples | OTC spot treatment | 3-5 days per lesion |
| Mild acne [mostly comedones] | OTC retinoid + niacinamide routine | 8-12 weeks |
| Moderate acne [regular pustules] | Dermatologist: topical prescription | 12-16 weeks |
| Severe acne [nodules/cysts] | Dermatologist: oral treatment likely | 4-6+ months |
When Professional Guidance Becomes Important
You can usually manage isolated pimples with over-the-counter products and basic skincare practices. However, certain situations indicate you should consult a dermatologist:
If you notice breakouts becoming more frequent or spreading to new areas, you are transitioning from occasional pimples to acne. Early intervention prevents the condition from worsening and reduces the risk of scarring.
Deep, painful nodules or cysts require professional treatment. These lesions form in the lower layers of skin and do not respond adequately to surface treatments. They carry high risk for permanent scarring and often need prescription medications or procedures.
When over-the-counter treatments fail to improve your skin after consistent use for six to eight weeks, stronger interventions may be necessary. Prescription retinoids, antibiotics, or hormonal therapies can address acne that does not respond to standard products.
Acne that affects your emotional wellbeing or daily life deserves attention regardless of clinical severity. Skin concerns that cause anxiety, embarrassment, or social withdrawal warrant professional support even if the physical condition seems mild.
Any signs of scarring, whether ice pick marks, raised tissue, or dark spots that persist for months, indicate you need guidance on treatment and prevention strategies.
How Do You Know If You Have Acne or Just Pimples? A Simple Self-Check
Not sure which one you're dealing with? Answer these five questions honestly. They won't replace a dermatologist's assessment, but they will give you a clear starting point.
Step 1: Count how many active lesions you have right now. One or two? Most likely isolated pimples. Three or more at different stages of healing and development? That pattern points toward acne.
Step 2: Look back at the last three months. Has your skin had stretches, two weeks or longer, where it was completely clear? If yes, you are probably dealing with pimples tied to identifiable triggers. If your skin has not been fully clear in three months or more, that persistent pattern is acne. Research published in the British Journal of Dermatology identifies persistent, multi-lesion breakouts over at least 12 weeks as a core diagnostic criterion for acne vulgaris.
Step 3: Map where they appear. Pimples can show up anywhere. Acne tends to concentrate on the face [forehead, nose, chin], chest, shoulders, and upper back, areas with the highest density of sebaceous glands. Lesions in multiple zones simultaneously are a strong signal for acne.
Step 4: Check the type of lesion. Are you seeing only whiteheads or red bumps? Or do you also have blackheads, deeper painful bumps that never come to a head, or cysts? A mix of lesion types, particularly non-inflamed comedones alongside inflamed papules and pustules, is a hallmark of acne, not isolated pimples.
Step 5: Note how your skin responds to basic care. A pimple treated with a spot product [benzoyl peroxide or salicylic acid] typically resolves within three to five days. If consistent OTC treatment for six to eight weeks has not meaningfully reduced your breakouts, you are most likely managing acne, and a dermatologist can assess whether you need a different approach.
What the pattern tells you
- Mostly yes answers: Isolated pimples. Focus on identifying your triggers.
- Mostly no answers: Likely acne. Consistent treatment and possibly professional evaluation are the right next steps.
- Mixed answers: Your skin may be in an early or transitional stage of acne. It is worth tracking it for another four to six weeks before deciding.
Frequently Asked Questions
Can a single pimple turn into acne?
One pimple will not transform into acne, but repeated pimples appearing in patterns may indicate developing acne. The distinction lies in frequency and underlying skin behavior rather than individual lesions. If breakouts become regular, your skin may be showing signs of the chronic dysfunction that characterizes acne-prone skin.
Should I treat occasional pimples differently than acne?
Yes. Spot treatment works for isolated pimples, while acne requires consistent application of products across affected areas to prevent new lesions. Treating only visible acne bumps allows microcomedones to continue forming, which is why a broader routine is different from learning how to treat pimples at home safely.
Can stress cause both pimples and acne?
Stress can trigger oil production and inflammation, which may cause an occasional pimple in anyone. In acne-prone skin, ongoing stress can worsen the existing breakout cycle and make acne feel more persistent. This is why understanding the connection between stress and pimples can help you manage triggers more clearly.
How long should I wait before considering my pimples to be acne?
If you experience regular breakouts for more than three months, with multiple lesions present most of the time, you are likely dealing with acne rather than occasional pimples. Persistent, recurring breakouts may need medical treatments for pimples or dermatologist guidance.
Do teenagers get acne while adults get pimples?
Both age groups can experience either condition. Teenagers commonly develop acne due to hormonal changes during puberty, but adults can also have acne triggered by hormones, stress, lifestyle, or skin type. Adults can also get occasional pimples without having chronic acne.
Will popping a pimple cause acne?
Popping a pimple will not directly cause acne, but it can spread bacteria to surrounding pores and increase inflammation, potentially creating more pimples nearby. It also damages tissue and increases the risk of marks or scars, so it helps to understand the difference between pimple marks vs scars.
Can acne go away on its own or will I always have it?
Some people experience acne only during certain life stages, especially adolescence, and naturally outgrow it as hormones stabilize. Others develop adult acne that needs ongoing management. The condition’s persistence depends on genetics, hormones, skin type, lifestyle, and the severity of the breakout cycle.
Is there a genetic difference between getting pimples versus acne?
Genetics strongly influences acne development. If your parents had acne, you may have a higher risk of developing the chronic condition rather than only occasional pimples. Genetic factors can affect sebum production, inflammation, and how your skin sheds cells.
Disclaimer
This information is published by Clear Ritual for educational purposes only and is not a substitute for professional medical advice. Skin responds differently from person to person and results vary. For persistent, painful, or scarring acne, consult a qualified dermatologist.
Sources:
- Zaenglein AL, et al. Acne vulgaris. Nature Reviews Disease Primers. 2015;1:15029.
- Tanghetti EA. The role of inflammation in the pathology of acne. Journal of Clinical and Aesthetic Dermatology. 2013;6[9]:27-35.
- Fitz-Gibbon S, et al. Propionibacterium acnes strain populations in the human skin microbiome associated with acne. Journal of Investigative Dermatology. 2013;133[9]:2152-2160.
- Bassett IB, et al. A comparative study of tea-tree oil versus benzoyl peroxide in the treatment of acne. Medical Journal of Australia. 1990;153[8]:455-458.
- Shahmoradi Z, et al. Comparison of topical 4% nicotinamide with 1% clindamycin in moderate acne vulgaris. International Journal of Dermatology. 2013;52[8]:999-1004.
- Williams HC, Dellavalle RP, Garner S. Acne vulgaris. The Lancet. 2012;379[9813]:361-372.
Editorial Standards
Clear Ritual has Strict sourcing guidelines to ensure our content is accurate and current. We rely on peer-reviewed studies, academic research institutions, and medical associations. We strive to use primary sources and refrain from using tertiary references. See a mistake? Learn More about our Editorial Standards.
Related Articles
Best Face Wash for Pimples: What to Look For
Published May 26, 2026
Best Ingredients to Treat Pimples (Salicylic Acid, Benzoyl Peroxide, etc.)
Published June 7, 2026

Boils vs Pimples: How to Know When It’s Something More Serious
Published June 6, 2026
Can Air Conditioner Cause Pimples? How AC Affects Your Skin
Published May 26, 2026