Atrophic vs Hypertrophic Acne Scars
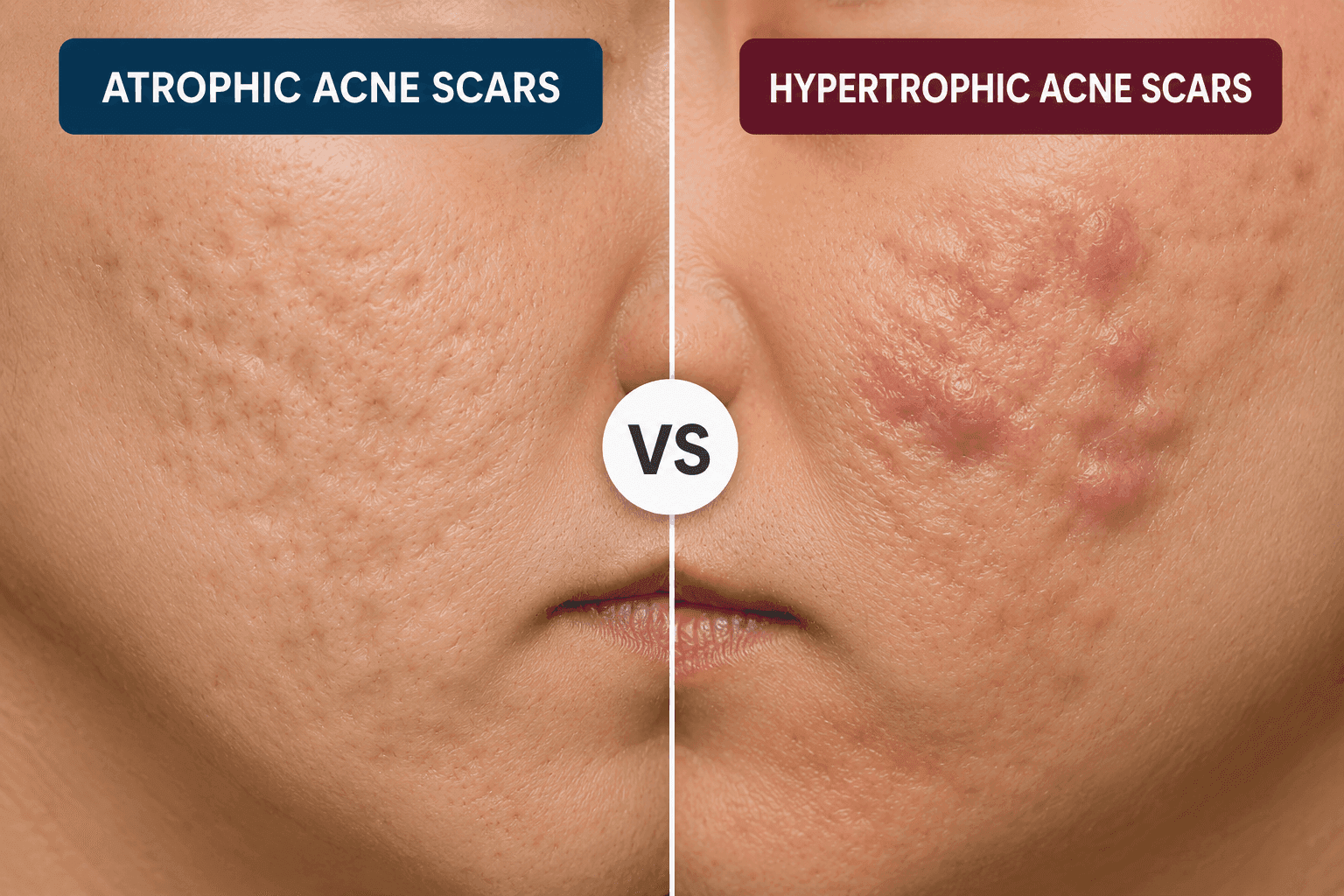
Atrophic and hypertrophic acne scars represent opposite extremes of the skin's wound-healing response following severe inflammatory acne breakouts. Atrophic scars are sunken or pitted depressions caused by a loss of collagen and supporting tissue during healing. In contrast, hypertrophic scars are raised, thickened bumps on the skin’s surface caused by an overproduction of collagen.
Treating acne scars depends heavily on whether they are atrophic or hypertrophic. While atrophic scars require procedures to stimulate collagen and restore lost volume, hypertrophic scars need therapies designed to flatten the raised tissue and calm overactive collagen production.
What Causes Atrophic vs Hypertrophic Scars?
Atrophic and hypertrophic scars are typically caused by skin damage based on how the body manages collagen production during the healing process.
Here are common triggers that cause these scars (which are not limited to acne):
| Atrophic Scars Causes | Hypertrophic Scars Causes |
|---|---|
| Severe cystic acne | Deep surgical incisions |
| Chickenpox infections | Thermal or chemical burns |
| Mole or cyst removals | Piercings or tattoos |
| Skin trauma with tissue loss | Infected or inflamed wounds |
| Genetic predisposition to poor wound healing | Wounds under high skin tension |
Difference Between Atrophic and Hypertrophic Acne Scars
Atrophic and hypertrophic acne scars are textural scarring, and they represent opposite healing responses by your body. The key difference is that atrophic scars appear as indentations due to collagen loss, while hypertrophic scars appear as raised tissue due to excess collagen.
Here are some key differences between atrophic and hypertrophic acne scars:
| Feature | Atrophic Scars | Hypertrophic Scars |
|---|---|---|
| Appearance | Sunken pits, craters, or depressions | Raised, firm bumps or thickened tissue |
| Collagen Level | Deficit (too little collagen produced) | Surplus (too much collagen produced) |
| Common Areas | Cheeks, temples, forehead, and nose | Jawline, chest, shoulders, and back |
| Main Goal | Build up skin volume and stimulate collagen | Flatten excess tissue and halt overproduction |
| Top Treatments | Microneedling, lasers, fillers, and TCA Cross | Steroid injections, silicone sheets, and cryotherapy |
Atrophic Scars vs Hypertrophic Scars Treatment
Atrophic and hypertrophic scars are caused by different processes and therefore require entirely different treatment approaches.
For hypertrophic scars (raised and thickened), the goal shifts to inhibiting and restructuring excess collagen, not stimulating more of it. Treatments that encourage collagen to fill in indentations are necessary to treat atrophic scars, which are sunken or depressed.
At-home treatments cannot totally eradicate atrophic or hypertrophic scars. To some extent, discolouration may be softened and faded with natural therapies. Dermatologists perform effective clinical therapies to eliminate or physically restructure scar tissue.
Atrophic Scars Treatment
Atrophic scars form when the skin loses tissue during healing and cannot rebuild enough collagen to restore the surface, making professional dermatological intervention the most effective route to treat them.
Some of the most common treatments for atrophic scars are:
Laser Resurfacing
CO2 lasers remove the outer skin layers, triggering the body to produce new collagen and resurfacing the skin.
Subcision
A fine needle is inserted beneath the scar to sever the fibrous bands tethering the skin downward, allowing the depressed surface to gradually lift.
Dermal Fillers
Dermal fillers are injected to temporarily lift depressed areas and restore volume to sunken areas.
Collagen-Stimulating Therapies
Procedures such as microneedling stimulate the body's natural production of collagen.
TCA Cross (Chemical Reconstruction of Skin Scars)
A high-concentration trichloroacetic acid solution is applied directly into the base of ice pick or boxcar scars to stimulate collagen and gradually fill the pit.
Hypertrophic Scars Treatment
Hypertrophic scars form when the body produces too much collagen during healing. They appear as firm, raised bumps, most commonly on the chest, back, and jawline.
Some common treatments done for hypertrophic scars are:
Intralesional Steroid Injections
To flatten elevated scars, corticosteroids (such as triamcinolone) are injected directly into the scars to break down extra collagen and reduce inflammation.
Silicone Gel or Sheet
Medical-grade silicone helps hydrate the skin, soften scar tissue, and gradually flatten elevated areas. It is frequently advised for both prevention and treatment.
Lasers and Cryotherapy
Liquid nitrogen is used in cryotherapy to freeze and reduce scar tissue. Pulsed Dye Lasers (PDL) effectively reduce redness, itching, and the blood vessel activity (vascularity) that keeps scars raised and inflamed.
Cryotherapy is often combined with steroid injections for better outcomes.
5-Fluorouracil (5-FU)
5-Fluorouracil (5-FU) is injected alongside steroids to suppress the overactive cells (fibroblasts) producing excess collagen, helping prevent the scar from thickening again.
Clear Ritual’s Perspective on Atrophic vs Hypertrophic Acne Scars
Clear Ritual emphasises that identifying scar type accurately is the most critical step in acne scar treatment. The Clear Ritual Skin Test helps assess your skin concerns and provides personalised insights that support accurate scar identification and treatment planning.
Our framework categorises scars based on how the skin heals, dividing them by collagen volume produced during healing.
Dealing with acne scars starts with distinguishing between two opposite types:
- Atrophic scars (depressed pits from collagen loss)
- Hypertrophic scars (raised bumps from excess collagen)
We believe the right treatment involves stimulating collagen via microneedling or lasers for pitted scars, while focusing on flattening raised scars with calming, non-stimulating methods.
Frequently Asked Questions
Are acne scars atrophic or hypertrophic?
Acne scars can be both, but they are predominantly atrophic or depressed. The type of scar depends on your skin type and how much collagen it produces after severe inflammatory acne.
What do Koreans do for acne scars?
Korean treatment for acne scars follows a highly structured, dual approach: advanced dermatological procedures and gentle, barrier-restoring at-home skincare.
The Korean routine focuses heavily on separating scar revision into addressing either the texture of indented pits or pigmentation, usually dark or red spots.
Do atrophic acne scars go away?
No, atrophic acne scars do not go away entirely on their own, and they can even appear deeper as skin tends to lose collagen with age.
However, these scars are not permanent. Professional dermatological treatments can significantly stimulate collagen production and smooth the skin's texture.
What is the hardest acne scar to fix?
The hardest scars to treat are ice pick scars (a deep type of atrophic scar) and keloid scars, a severe form of raised scarring that extends beyond the original wound and tends to recur even after removal.
Do atrophic scars flatten over time?
Atrophic scars do not flatten or fill in on their own over time. Because they form when the skin loses tissue and collagen during healing, they are generally permanent and require cosmetic or dermatological intervention to improve their appearance.
How to treat an atrophic scar?
Flattening an atrophic scar with at-home skincare like retinoids can aid remodelling. Professional dermatological procedures, such as microneedling, fractional laser resurfacing, or dermal fillers, are the most effective methods for raising the indentation to the level of the surrounding skin.
Will a hypertrophic scar ever go away?
While a hypertrophic scar rarely disappears completely without intervention, it often flattens, softens, and fades significantly on its own within one to two years.
Because these scars stay within the boundaries of the original injury, they respond very well to dermatological treatments.
References
- https://pmc.ncbi.nlm.nih.gov/articles/PMC2958495/
Editorial Standards
Clear Ritual has Strict sourcing guidelines to ensure our content is accurate and current. We rely on peer-reviewed studies, academic research institutions, and medical associations. We strive to use primary sources and refrain from using tertiary references. See a mistake? Learn More about our Editorial Standards.