Types of Acne Scars: Ice Pick, Boxcar & Rolling

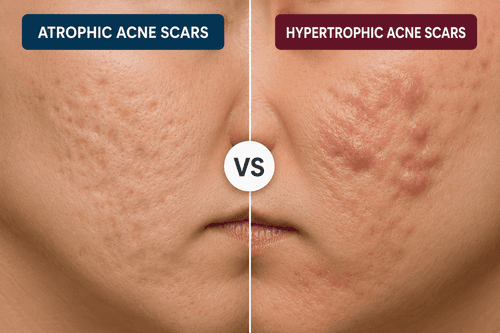
Not all acne scars are the same — and that distinction matters more than most people realise. The three main types of acne scars (ice pick, boxcar, and rolling) are all atrophic scars, meaning they sit below the surface of surrounding skin because the skin lost collagen during healing. Each type has a distinct shape, depth, and mechanism — and each responds differently to treatment.
Atrophic acne scars are depressed scars that form when the skin produces too little collagen to fully repair a site of inflammatory damage. They are permanent structural changes in the dermis — not surface discolouration, which fades on its own.
At a glance:
- Ice pick scars — narrow, deep pits smaller than 2mm across; the hardest type to treat
- Boxcar scars — wider, angular depressions with sharp edges; 1.5–4mm across
- Rolling scars — broad, wave-like indentations caused by fibrous tethering beneath the skin
- Mixed scarring — most people have more than one type in the same area
- Post-inflammatory hyperpigmentation (PIH) — flat dark marks that are not scars and do fade without structural treatment
Acne scars form when inflamed breakouts damage the skin's deeper layers, disrupting normal collagen production during healing. The three main types - ice pick, boxcar, and rolling scars - differ in shape and depth, each resulting from how your skin attempted to repair itself after inflammatory acne lesions.
Key Takeaways:
- Ice pick scars are narrow, deep pits that extend into the dermis
- Boxcar scars have wider, angular depressions with defined edges
- Rolling scars create wave-like indentations from tethering beneath the skin
- Scar type depends on inflammation severity and individual healing response
- Different scar types often require different treatment approaches
What Happens When Acne Leaves Scars
Not every pimple leaves a scar. Scarring occurs when inflammation penetrates deep enough to damage the structural support network in your dermis. When your skin attempts to heal, it may produce too little collagen, creating depressed scars, or occasionally too much, forming raised scars.
The likelihood of scarring increases with several factors. Picking or squeezing inflamed lesions forces bacteria and debris deeper into surrounding tissue, expanding the zone of damage. Delayed treatment of severe inflammatory acne gives inflammation more time to destroy collagen and elastin fibers. Your individual healing response, influenced by genetics and overall skin health, also determines whether damaged tissue repairs smoothly or leaves permanent textural changes.
Ice Pick Scars: Deep and Narrow
Ice pick scars appear as small, deep holes in the skin, resembling puncture marks from a sharp tool. They extend vertically into the dermis, sometimes reaching the deeper reticular dermis layer. These scars typically measure less than 2 millimeters in diameter but can be quite deep relative to their width.
These scars develop most commonly from deep inflammatory acne like papules or cysts. When intense inflammation destroys tissue in a concentrated area, the healing process creates a narrow column of damaged tissue. The skin surface tries to close over this deep void, but without adequate collagen support underneath, a deep pit remains.
Ice pick scars most frequently appear on the cheeks and forehead, where skin is thinner and inflammatory acne tends to concentrate. Their depth makes them particularly challenging to address, as topical treatments cannot reach the base of the scar where new collagen formation would be needed.
Boxcar Scars: Angular Depressions
Boxcar scars present as round or oval depressions with sharply defined vertical edges, similar to chickenpox scars. Unlike ice pick scars, they are wider - typically 1.5 to 4 millimeters across - and create a box-like appearance in cross-section. These scars vary in depth, with shallow boxcar scars responding better to treatment than deeper variants.
These scars form when inflammatory acne destroys collagen over a wider area than ice pick scars. During healing, the skin surface becomes tethered to deeper structures, but the loss of volume creates a broad depression. The sharp edges result from complete loss of tissue at the depression's perimeter, leaving an abrupt transition between normal skin and scarred areas.
Boxcar scars commonly develop on areas with thicker skin, particularly the lower cheeks and jawline. They often appear in clusters, especially in people who experienced widespread inflammatory acne. The angular edges distinguish them from rolling scars, which have gentler slopes.
Rolling Scars: Wave-Like Indentations
Rolling scars create an undulating, wave-like appearance across the skin surface. They are typically wider than other atrophic scars - usually 4 to 5 millimeters or more - and have sloped edges rather than sharp borders. The skin appears to roll between normal areas and depressed zones, creating shadows that become more noticeable in certain lighting.
These scars develop through a different mechanism than ice pick or boxcar scars. Fibrous bands form beneath the skin surface, pulling the epidermis downward and tethering it to deeper subcutaneous tissue. This creates broad depressions without the tissue loss seen in other scar types. The inflammation that triggers rolling scars may have been less intense but more widespread, affecting larger areas of dermal tissue.
Rolling scars predominantly affect the cheeks and jawline. They can make the skin texture appear uneven and aged, as the wave-like surface disrupts how light reflects off the face. These scars often coexist with other types, creating complex textural irregularities.
Comparing the Three Main Scar Types
| Scar Type | Width | Depth | Edge Definition | Common Location | Formation Cause |
|---|---|---|---|---|---|
| Ice Pick | Very narrow (<2mm) | Very deep | Pointed bottom | Cheeks, forehead | Deep inflammatory lesions destroying tissue in narrow column |
| Boxcar | Moderate (1.5–4mm) | Varies | Sharp, vertical | Lower cheeks, jawline | Wider area of collagen loss with defined borders |
| Rolling | Wide (4mm+) | Shallow to moderate | Sloped, gradual | Cheeks, jawline | Fibrous tethering pulling skin downward |
Treatment Approaches by Scar Type: What Actually Works
Different scar types respond to different interventions because they have different physical structures. Ice pick scars need treatments that reach deep into the dermis. Rolling scars need subcision to release fibrous tethering. Boxcar scars often respond well to volume-restoring or resurfacing approaches.
Treatment Options at a Glance
| Treatment | Best For | How It Works | Typical Sessions | Home or Professional |
|---|---|---|---|---|
| TCA CROSS | Ice pick scars | High-concentration acid applied to scar base triggers focused collagen rebuild | 3–6 sessions, 4–6 weeks apart | Professional only |
| Subcision | Rolling scars | Needle breaks fibrous bands tethering skin downward | 2–4 sessions | Professional only |
| Microneedling (RF) | Boxcar + rolling scars | Micro-injuries stimulate collagen; RF version adds heat for deeper remodelling | 3–6 sessions | Professional (RF); at-home rollers for maintenance only |
| Fractional laser (CO₂ or Erbium) | All types, especially boxcar | Ablates scar tissue in micro-columns, triggers wholesale collagen remodelling | 2–4 sessions | Professional only |
| Dermal fillers | Rolling + boxcar scars | Hyaluronic acid or biostimulators physically lift the depression | 1–2 sessions (temporary) | Professional only |
| Chemical peels (glycolic, TCA) | Shallow boxcar, surface texture | Removes damaged surface layers, encourages new skin formation | Series of 4–6 | Professional; milder acids at home |
| Topical retinoids | All types (adjunct) | Stimulate fibroblast activity and new collagen synthesis over months | Daily, long-term | At-home with dermatologist guidance |
Why Ice Pick Scars Are the Hardest to Treat
Ice pick scars are narrow tunnels that extend deep into the reticular dermis. Most resurfacing treatments — lasers, peels, needling — work across the skin surface and cannot reliably deliver energy or stimulus to the base of a sub-2mm tunnel. TCA CROSS (chemical reconstruction of skin scars) is the exception: it delivers a high-concentration acid specifically to the floor of each scar, triggering a focal inflammatory response that builds collagen from the bottom up.
What You Can Start at Home
Home care cannot structurally alter established scars, but it can meaningfully support professional treatment outcomes and slow new scar formation:
- Vitamin C serum (ascorbic acid 10–20%) — supports collagen synthesis and reduces post-inflammatory hyperpigmentation alongside scars
- Retinol or retinaldehyde — promotes skin cell turnover and fibroblast activity; start low (0.025–0.05%) and increase gradually
- Broad-spectrum SPF 30+ — daily UV protection prevents hyperpigmentation from worsening the visual contrast of scars
- Niacinamide (5–10%) — reduces inflammation and PIH; well-tolerated even on sensitive post-acne skin
- Avoid physical exfoliation over active scars — scrubs and rough tools cause micro-trauma that can worsen textural irregularity
Why Some People Scar More Than Others
Individual scarring risk varies significantly based on multiple interacting factors. Genetics influence how your immune system responds to P. acnes bacteria and how efficiently your fibroblasts produce collagen during wound healing. Some people naturally produce less organized collagen matrices, increasing depression risk, while others overproduce collagen, leading to raised scars.
The inflammatory response itself determines damage severity. Higher levels of inflammatory mediators like cytokines and matrix metalloproteinases break down more collagen and elastin. Prolonged inflammation gives these destructive processes more time to work. Stress elevates cortisol, which can amplify inflammatory pathways and impair healing efficiency.
Melanin-rich skin faces additional considerations. While all skin types can develop atrophic scars, darker skin tones have higher risk for post-inflammatory hyperpigmentation and keloid formation. The increased melanocyte activity that provides natural sun protection can also trigger excess pigment production around healing sites.
Lifestyle factors modify scarring risk through multiple pathways. Poor sleep disrupts growth hormone release needed for tissue repair. High-glycemic diets trigger insulin spikes that promote inflammation. Smoking reduces oxygen delivery to healing tissue and impairs fibroblast function. Inadequate protein intake limits the amino acid building blocks needed for collagen synthesis.
The Role of Inflammation and Healing
The deeper and longer inflammation persists, the more likely scarring becomes. When a pore becomes blocked with sebum, dead skin cells, and bacteria, the resulting pressure can rupture the follicle wall. This spills inflammatory contents into the surrounding dermis, triggering an immune response.
Your immune cells release enzymes to fight infection, but these same enzymes damage the collagen framework supporting skin structure. As inflammation resolves, fibroblasts migrate to the damaged area to deposit new collagen. However, this repair collagen often differs in organization from the original basket-weave pattern, creating irregular texture.
The balance between collagen breakdown and synthesis determines the final scar appearance. Insufficient collagen production relative to the amount destroyed creates depressions - atrophic scars like ice pick, boxcar, and rolling types. Excessive collagen production creates raised scars - hypertrophic scars or keloids. Most facial acne scars are atrophic because facial skin has less tendency toward overproduction.
Picking or manipulating inflamed lesions dramatically worsens this process. Manual pressure forces inflammatory material deeper and wider into tissue, expanding the damage zone. Introducing surface bacteria into deeper layers increases infection risk. Breaking the skin barrier triggers more aggressive inflammatory cascades. The mechanical trauma itself destroys additional tissue that must then heal.
What the Research Says: Atrophic Scar Formation
The science behind acne scarring is well-established. Here is what the clinical evidence shows:
Prevalence: Approximately 95% of people with acne develop some degree of scarring, with atrophic scars accounting for the vast majority of cases — studies estimate 80–90% of acne scars are atrophic rather than hypertrophic. [1]
Collagen destruction: Research published in the Journal of Investigative Dermatology has shown that inflammatory mediators — particularly matrix metalloproteinases (MMPs) — break down existing collagen in the dermis during the acute inflammatory phase of a breakout. The more severe and prolonged the inflammation, the greater the MMP activity and the deeper the collagen loss. [2]
Healing timeline: Wound-healing research establishes that the dermis remodels for up to 12–18 months after initial damage. This means scar appearance can continue to change — sometimes improving slightly — for over a year without any intervention. [3]
Picking worsens outcomes: A 2022 study in Dermatology and Therapy found that patients who reported regular acne excoriation (picking or squeezing) had significantly higher rates of moderate-to-severe atrophic scarring compared to those who did not. [4]
Skin tone and scarring risk: Research consistently shows that individuals with Fitzpatrick skin types IV–VI face higher risk of concurrent post-inflammatory hyperpigmentation alongside atrophic scars, which increases the visibility of scarring even when textural depth is similar to lighter skin tones. [5]
Sources: [1] Fabbrocini G, et al. Acne scarring treatment using skin needling. Clin Cosmet Investig Dermatol. 2010. [2] Holland DB, et al. Inflammatory events are involved in acne lesion initiation. J Invest Dermatol. 2004. [3] Gurtner GC, et al. Wound repair and regeneration. Nature. 2008. [4] Tan J, et al. Acne excoriée: prevalence and psychological burden. Dermatol Ther. 2022. [5] Davis EC, Callender VD. Postinflammatory hyperpigmentation. J Clin Aesthet Dermatol. 2010.
Early Prevention Strategies
Preventing scars starts with managing inflammatory acne before deep tissue damage occurs. Early intervention reduces the inflammation duration and intensity that drive scarring. Gentle cleansing removes excess oil and debris without stripping the skin barrier, which would trigger compensatory oil production and inflammatory signaling.
The skin barrier plays a central protective role. When compromised by harsh products, over-exfoliation, or excessive washing, transepidermal water loss increases and barrier repair lipids become depleted. This barrier disruption allows deeper penetration of irritants and makes inflammatory responses more severe. Maintaining barrier integrity through appropriate hydration and avoiding over-stripping helps contain inflammation to superficial layers.
Sun protection serves multiple protective functions. UV radiation triggers inflammatory mediators that can worsen active acne inflammation. It also interferes with normal collagen remodeling during healing, potentially increasing scar severity. In darker skin tones, UV exposure intensifies post-inflammatory hyperpigmentation that often accompanies scars, making them more noticeable even after texture improvements.
Resisting the urge to pick or squeeze inflamed lesions cannot be overstated. The temporary satisfaction of extraction creates significantly worse long-term outcomes. If you struggle with skin picking, keeping hands busy with stress balls or fidget tools, covering mirrors during high-risk times, and addressing underlying anxiety can help break the cycle.
When Different Scars Require Professional Assessment
Recognizing when home management reaches its limits helps prevent worsening and frustration. If you notice scars deepening or multiplying despite consistent gentle care, professional evaluation becomes important. Severe inflammatory acne that creates painful nodules or cysts beneath the skin frequently requires intervention beyond topical approaches to prevent extensive scarring.
Scars that significantly impact your confidence or daily life warrant professional discussion regardless of clinical severity. The psychological burden of visible scarring affects quality of life, and various professional treatments can improve texture and appearance. Earlier professional intervention for active inflammatory acne also prevents new scar formation.
Certain warning signs indicate deeper issues needing medical attention. Acne accompanied by fever, rapidly spreading redness, or severe pain may indicate infection requiring prompt treatment. Sudden onset of severe acne in adulthood sometimes signals hormonal imbalances or other systemic conditions. Acne that fails to respond to multiple well-formulated approaches over several months suggests the need for prescription options or investigation of underlying triggers.
What This Means for You
By understanding which type of acne scar you have — and the mechanism behind it — you can make smarter decisions about where to invest time, money, and skin care effort. Most people with atrophic scarring see meaningful improvement within 3–9 months of a structured approach that matches treatment to scar type, rather than applying generic solutions to all scars equally.
Your next actions:
- Identify your dominant scar type using the raking-light and skin-stretch test described above
- Photograph your skin monthly in consistent lighting to track changes objectively
- Start a retinoid + vitamin C + SPF routine if you haven't — these are the best-evidenced at-home adjuncts to any professional treatment plan
- Prioritise stopping new scar formation by managing active inflammatory acne first; new scars compound existing textural irregularity
- Book a professional consultation if you have ice pick scars, if scarring is emotionally distressing, or if three months of consistent home care has produced no improvement
If your acne continues to flare despite a consistent skincare approach — creating new scars faster than existing ones can be treated — the internal triggers (hormonal, dietary, stress-related, or microbiome-driven) may need to be addressed alongside surface care. A structured skin assessment helps identify which internal factors are driving your individual pattern, so treatment can work from the inside out as well as the outside in.
Can ice pick scars go away on their own?
Ice pick scars are permanent structural changes in the dermis and do not resolve without intervention. Their depth means the skin cannot naturally regenerate the lost tissue or fill the depression. Professional treatments that stimulate collagen production in the scar base or physically modify scar architecture are typically needed for improvement.
Which type of acne scar is hardest to treat?
Ice pick scars generally present the greatest treatment challenge due to their depth and narrow diameter. Their vertical tunnel shape makes it difficult for treatments to reach the scar base where collagen remodeling needs to occur. Boxcar and rolling scars, being shallower or caused by tethering rather than tissue loss, often respond better to various interventions.
Do rolling scars get worse with age?
Rolling scars can become more noticeable with age as natural collagen and elastin degradation reduces skin firmness and volume. The fibrous bands causing rolling scars remain constant, but as surrounding tissue loses structural support, the depressions may appear deeper and the wave-like texture more pronounced. This makes earlier intervention potentially more effective.
Can you have multiple types of acne scars at once?
Most people with acne scarring have a combination of scar types rather than just one. Different inflammatory lesions heal differently even on the same person, creating ice pick, boxcar, and rolling scars in various facial areas. This mixed scarring often requires combination treatment approaches tailored to the specific scar types present.
How long after acne clears do scars form?
Scars form during the healing process itself, typically becoming apparent within weeks to months after the inflammatory lesion resolves. The scar may continue remodeling for up to 12–18 months after initial healing, during which texture and depth can change somewhat. What appears as a scar after six months will likely represent permanent textural change.
Does skin type affect what kind of acne scars you get?
Skin type influences scarring patterns more through healing tendencies than scar type. All skin types can develop ice pick, boxcar, and rolling scars. However, darker skin tones have higher risk for keloid and hypertrophic (raised) scars and post-inflammatory hyperpigmentation alongside atrophic scars. Oily skin types may experience more inflammatory acne, increasing overall scarring risk.
Can new acne scars form on top of old ones?
New inflammatory acne lesions can certainly occur in previously scarred areas, potentially creating additional scarring or worsening existing scars. Areas with compromised skin structure from previous scarring may actually be more vulnerable to new inflammatory damage. This underscores the importance of managing active acne even after some scarring has occurred.
Are acne scars and acne marks the same thing?
Acne scars and marks are different. Scars involve permanent textural changes from dermal damage - depressions like ice pick, boxcar, and rolling scars, or raised areas like keloids. Marks, also called post-inflammatory hyperpigmentation or erythema, are flat discolorations that fade over months to years without textural change. Marks represent pigment or blood vessel changes without structural skin damage.
How to Tell What Type of Acne Scar You Have
You can identify your scar type using natural lighting and a simple self-examination. The key is to look at shape, depth, and edge definition — the three physical features that reliably distinguish one scar type from another.
Step 1: Find natural, raking light Side-angled light (from a window, not overhead) casts shadows that reveal depth and texture far more clearly than direct or diffuse lighting. This is the same lighting technique dermatologists use in clinical photography.
Step 2: Look at the edges
●Sharp, steep, almost cliff-like edges → likely boxcar
●Pointed bottom that narrows as it goes deeper, like a pinhole → likely ice pick
●Gradual, sloping edges that blend into surrounding skin → likely rolling
Step 3: Assess the width
●Smaller than a pinhead (under 2mm) → ice pick
●Wider than a pencil eraser mark (1.5–4mm) → boxcar
●Larger, covering 4mm or more with an undulating surface → rolling
Step 4: Press the skin gently sideways Push the skin to either side of the depression with two fingertips. Rolling scars partially flatten when the skin is stretched — because they are caused by fibrous tethering, not tissue loss. Ice pick and boxcar scars do not flatten.
Step 5: Accept that you probably have more than one type Mixed scarring is the norm. A cheek with widespread acne history may have ice pick scars near the nose, boxcar scars along the lower cheek, and rolling scars toward the jawline — all at once. Identifying the dominant type guides your first treatment priority.
When in doubt, photograph your skin in the same raking light every month. Changes in texture are easier to track across time than to assess in a single observation.
What to Expect: Acne Scar Timeline
Realistic expectations matter — both for mental wellbeing and for knowing when a treatment is working vs when to reassess.
Without treatment (natural remodelling only):
- Weeks 1–4: Active inflammation resolves; PIH (flat dark marks) begins to appear and is often mistaken for scarring
- Months 1–6: Natural collagen remodelling occurs; very shallow atrophic scars may improve marginally; deep ice pick and boxcar scars do not resolve
- Months 6–18: The skin's remodelling window closes; what remains after 12–18 months is likely permanent without intervention
- Takeaway: Flat marks (PIH) fade. Textural scars do not heal on their own.
With professional treatment:
- TCA CROSS for ice pick scars: Most patients see 50–70% depth reduction after 3–6 sessions over 4–6 months [1]
- Subcision for rolling scars: Visible improvement often appears after session 1–2; full benefit at 3–4 months post final session
- Fractional laser: Skin may look worse for 7–14 days post-treatment (redness, swelling, peeling); improvement in texture becomes apparent at 4–8 weeks; optimal results at 6 months
- Microneedling: Gradual improvement over 3–6 months after completing a 3–6 session course; more suitable for rolling and shallow boxcar scars than ice pick
With consistent at-home adjunct care (retinoids + vitamin C + SPF):
- Weeks 4–8: Reduction in PIH contrast; skin tone begins to even
- Months 3–6: Modest improvement in very shallow surface texture; retinoids are not capable of reversing established atrophic scars but improve surrounding skin quality
- Months 6–12: If combined with professional treatment, home-care accelerates recovery between sessions
Most people with moderate-to-severe atrophic scarring see the clearest improvement between month 3 and month 9 of a structured treatment plan — not in the first few weeks.
[1] Bhardwaj D, et al. TCA CROSS in the treatment of ice pick acne scars. J Cutan Aesthet Surg. 2021
Frequently Asked Questions
Can I use retinol directly on acne scars?
Yes — retinol is safe to apply over atrophic acne scars and is one of the most evidence-backed at-home ingredients for supporting scar improvement. It works by stimulating fibroblast activity and accelerating skin cell turnover, which gradually improves surface texture. Start with a low concentration (0.025–0.05%), use it at night only, and always follow with SPF the next morning. It will not erase established ice pick or boxcar scars but meaningfully improves overall skin quality around them.
How is a rolling scar different from just uneven skin texture?
Rolling scars have a specific cause: fibrous bands beneath the skin that physically pull the epidermis downward, creating wave-like depressions. You can distinguish them from general uneven texture by stretching the skin sideways with two fingertips — rolling scars partially flatten because the tethering relaxes, whereas general uneven texture does not change when stretched. This physical test also helps explain why subcision (cutting the fibrous bands) is the primary professional treatment for rolling scars.
Will acne scar treatments make things look worse before they get better?
Yes — most professional treatments involve a temporary worsening before improvement. Fractional laser causes 7–14 days of redness and peeling. Subcision typically produces bruising and swelling for 5–10 days. TCA CROSS causes temporary scabbing at each treated scar site over 1–2 weeks. This is not a sign that the treatment has failed; it is the visible phase of the healing and collagen-building response the treatment triggered. Results become apparent weeks to months after the inflammatory phase settles.
Does diet affect how visible my acne scars look?
Diet does not change the structural depth of existing scars, but it can affect how visible they appear. High-glycemic foods promote chronic low-level inflammation that worsens post-inflammatory hyperpigmentation — the flat dark marks that sit alongside scars and increase their visual contrast. Anti-inflammatory foods rich in vitamins C and E support collagen synthesis, which may marginally improve skin quality around scars over time. Hydration also affects skin plumpness; well-hydrated skin makes atrophic depressions appear slightly less deep.
At what point should I stop active skincare and see a dermatologist about my scars?
If you have been consistent with a gentle, science-backed skincare routine — including a retinoid, vitamin C, and daily SPF — for 3–6 months and see no improvement in scar texture, professional evaluation is the logical next step. This is also the right threshold if scarring is causing significant emotional distress, if you have deep ice pick scars (which do not respond to topical care), or if active inflammatory acne is continuing to form new scars despite your routine. Earlier professional intervention typically yields better outcomes.
Can the same acne scar change type over time?
Scars do not convert from one type to another, but their appearance can shift with age. Rolling scars become more noticeable as natural collagen loss reduces skin firmness — the fibrous bands remain constant while surrounding tissue loses volume, making depressions look deeper. Boxcar scars similarly become more pronounced with age-related skin thinning. Ice pick scars are the most stable in appearance but do not self-resolve. Natural ageing does not improve atrophic scars without intervention.
Is there a difference between acne scars on darker skin tones vs lighter skin tones?
The three scar types (ice pick, boxcar, rolling) occur in all skin tones. The key difference is that individuals with Fitzpatrick skin types IV–VI are significantly more prone to concurrent post-inflammatory hyperpigmentation (PIH) — flat dark marks that develop alongside atrophic scars and increase their overall visual impact. Darker skin tones also carry higher risk of keloid formation (raised scars) from inflammatory acne. Treatment protocols for darker skin require modified laser settings and additional caution to avoid triggering further hyperpigmentation.
How do I know if what I'm seeing is a scar or just a post-acne mark?
Run your fingertip lightly across the area in question. If the skin feels completely flat and the discolouration is the only change — it is a post-inflammatory mark (PIH or erythema), not a scar. PIH fades over months with consistent SPF and vitamin C use. If you feel a depression or texture change, even a subtle one, that is structural scarring. The two often occur together — a depressed scar surrounded by flat hyperpigmentation — which makes them harder to distinguish visually. Lighting at a low angle (raking light) makes textural depressions visible even when PIH is present.
Editorial Standards
Clear Ritual has Strict sourcing guidelines to ensure our content is accurate and current. We rely on peer-reviewed studies, academic research institutions, and medical associations. We strive to use primary sources and refrain from using tertiary references. See a mistake? Learn More about our Editorial Standards.